Normal Pressure Hydrocephalus: Gait, Cognition, and Shunts Explained
 Jan, 28 2026
Jan, 28 2026
When an older adult starts walking like they’re stuck in mud-feet dragging, steps wide and unsteady-and begins forgetting names or losing bladder control, it’s easy to assume it’s just aging. But what if it’s not? What if it’s something treatable? That’s the reality of normal pressure hydrocephalus (NPH), a neurological condition that mimics dementia but can be reversed with surgery. It’s not rare. It’s underdiagnosed. And for many, it’s the difference between living in a nursing home and walking again.
What Exactly Is Normal Pressure Hydrocephalus?
Normal pressure hydrocephalus happens when too much cerebrospinal fluid (CSF) builds up in the brain’s ventricles-the fluid-filled spaces inside the brain. Unlike other forms of hydrocephalus where pressure spikes dangerously, NPH keeps pressure within the normal range: between 70 and 245 mm H₂O. That’s why it’s called “normal pressure.” The problem isn’t pressure-it’s volume. The fluid swells the ventricles, squeezing nearby brain tissue and disrupting signals that control walking, thinking, and bladder function.
This condition mostly hits people over 60. About 0.4% of everyone over 65 has it. In nursing homes, that number jumps to nearly 6%. And here’s the kicker: up to 60% of these cases get mistaken for Alzheimer’s or Parkinson’s. That’s because the symptoms look almost identical. But unlike those diseases, NPH doesn’t always get worse over time. With the right treatment, many people get their lives back.
The Three Signs: Gait, Cognition, and Bladder Control
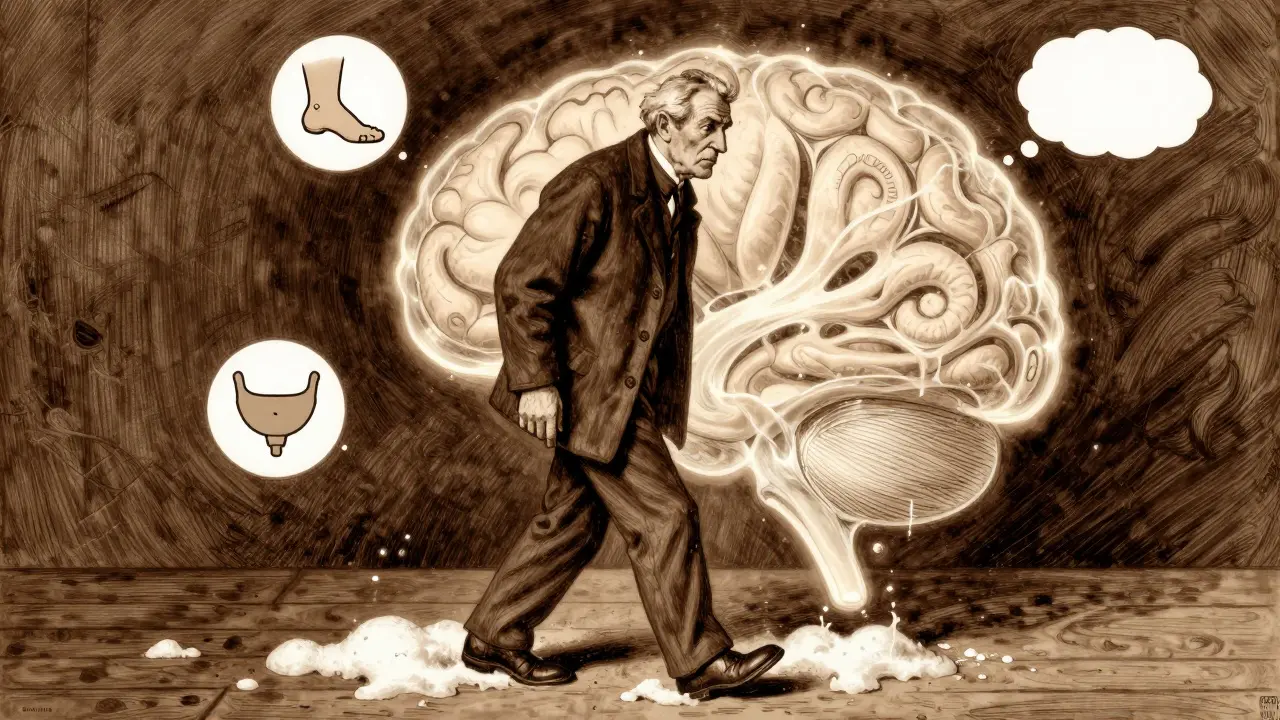
NPH has a classic trio of symptoms, often called the “triad.” But not everyone gets all three. In fact, only about 30% of patients show all of them at once. Most start with one-and that’s where diagnosis gets tricky.
- Gait disturbance: This is the most common and earliest sign. People walk slowly, with short, shuffling steps. Their feet seem glued to the floor. They might turn in small, stiff movements. It’s not like Parkinson’s tremors-it’s more like walking through deep snow. In studies, nearly 100% of diagnosed NPH patients have this symptom. A timed 10-meter walk test can show how bad it is. If someone takes more than 20 seconds to walk 10 meters, it’s a red flag.
- Cognitive impairment: Memory loss? Yes. But it’s not the kind you see in Alzheimer’s. NPH affects executive function: planning, focusing, starting tasks, remembering why you walked into a room. People sound confused, slow to respond, or stuck on one thought. Neuropsych tests like the Trail Making Test or Digit Symbol Substitution Test show clear deficits. About 73% of patients have this symptom, but it often gets written off as “just getting older.”
- Urinary incontinence: This usually comes later. It starts with urgency-needing to go suddenly-and progresses to accidents. It’s not about weak muscles. It’s the brain losing its ability to signal the bladder. Only about one-third of patients have this at diagnosis, but it’s a major sign when it shows up with gait and thinking problems.
These symptoms develop slowly-over months or even years. That’s why they’re missed. People think, “He’s just getting frail.” But if you catch it early, you can change the outcome.
How Do Doctors Diagnose It?
There’s no single blood test for NPH. Diagnosis needs a mix of imaging, tests, and observation. First, doctors check for enlarged ventricles on a CT scan or MRI. The Evan’s index-a ratio of ventricle width to brain width-must be 0.3 or higher. MRI also shows periventricular edema, a telltale sign of fluid buildup pressing on brain tissue.
Then comes the CSF tap test. A needle is inserted into the lower back to remove 30-50 mL of spinal fluid. That’s about two cups. Right after, doctors measure walking speed, balance, and thinking ability. If the person walks 10% faster or scores better on a memory test, that’s a strong sign they’ll respond to a shunt. Studies show this test predicts shunt success with 82% accuracy.
Some centers use a more advanced test: external lumbar drainage. A catheter stays in the spine for 2-3 days, draining fluid continuously. If symptoms improve during that time, the chance of success with a shunt jumps to 89%. This isn’t available everywhere, but where it is, it’s gold standard.
Doctors also rule out other causes. Alzheimer’s shows different brain patterns on MRI. Parkinson’s has tremors and stiffness in limbs. Vascular dementia has a history of strokes. NPH doesn’t. That’s why specialists stress: if someone over 60 has gait trouble plus cognitive changes, NPH should be on the list-even if they’ve already been told it’s “just dementia.”
Shunt Surgery: The Only Treatment
There’s no pill for NPH. No drug slows it down. The only proven treatment is surgery: a ventriculoperitoneal (VP) shunt. It’s a thin tube placed in the brain’s ventricle, connected to another tube that runs under the skin to the abdomen. A valve in between controls how much fluid drains-usually set between 50 and 200 mm H₂O. The fluid gets absorbed naturally by the body.
The surgery takes about an hour under general anesthesia. Most people go home in 2-3 days. Recovery takes 6-12 weeks. But the turnaround can be fast. Some patients report walking better within 48 hours. One man on a patient forum said his 10-meter walk dropped from 28 seconds to 12 seconds after surgery. Another regained bladder control after 18 months of accidents.
Success rates? 70-90% of properly selected patients improve. That’s better than most Alzheimer’s drugs, which help only about 35% of users. But not everyone responds. About 20-30% of shunts don’t help-sometimes because the diagnosis was wrong, or the brain has too much damage from years of untreated fluid buildup.
Risks and Complications
Shunts save lives-but they’re not risk-free. The most common problems:
- Infection: Happens in about 8.5% of cases. More common in people over 80.
- Shunt malfunction: One in six shunts fails within two years. It can clog, break, or drain too much or too little.
- Subdural hematoma: Bleeding between the brain and skull. Occurs in about 5.7% of cases.
- Overdrainage: Too much fluid removed can cause headaches, nausea, or even collapse of the ventricles.
Most complications can be fixed. A valve can be adjusted. A blocked tube can be replaced. But the key is follow-up. Patients need check-ins at 2 weeks, 6 weeks, 3 months, and 6 months after surgery. Many need one or two revisions over their lifetime.
Why Is NPH So Often Missed?
Because it looks like other diseases. And because doctors aren’t trained to think of it. A 2022 study found that 60% of NPH cases are misdiagnosed. Many patients wait over a year before getting the right test. Insurance often denies the CSF tap test or lumbar drainage-37% of claims get rejected. That delays diagnosis, and delay reduces success.
Dr. Norman Relkin from Weill Cornell says NPH is “the great masquerader of geriatric neurology.” It hides in plain sight. A 72-year-old who can’t walk or remember his grandkids? He’s not just aging. He might be able to walk again.
Also, many patients have mixed conditions. About 25-30% of NPH cases come with Alzheimer’s or vascular dementia. That makes diagnosis harder. But studies show that even in mixed cases, shunt surgery still improves gait and function. The key is not to give up because “it’s too complicated.”
What’s New in NPH Research?
Things are changing fast. In 2022, the FDA approved a new device called the Radionics® CSF Dynamics Analyzer. It measures how well the brain drains fluid-giving doctors a precise number instead of guessing. That’s raised diagnostic accuracy to 89%.
There’s also a new app, the iNPH Diagnostic Calculator, based on Japanese guidelines. You plug in 12 symptoms and test results, and it gives a percentage chance of shunt success-85% accurate.
Researchers are now testing blood and spinal fluid biomarkers. Three clinical trials are underway looking for proteins that only appear in NPH. Early results show 92% sensitivity. If they work, we could have a simple blood test in the next few years.
And the shunt market is growing. Medtronic, Codman, and Miethke make the main devices. Medicare pays about $28,500 per surgery. But access is uneven. Rural areas often don’t have neurosurgeons trained in NPH. That’s why awareness matters.
What Happens After Surgery?
Most people see big improvements. A 2022 survey of 457 NPH patients found:
- 76% improved walking
- 62% had better thinking
- 58% regained bladder control
- 89% said they were satisfied with their outcome
But it’s not perfect. About one-third needed a shunt revision. Some had chronic headaches. Others didn’t improve cognitively, even with good gait recovery. That’s why patient selection is everything. If the tap test doesn’t help, the shunt probably won’t either.
Recovery takes time. Physical therapy helps. Occupational therapy helps. Family support matters. Many patients go from needing help to walk to driving again, cooking meals, or traveling to see grandchildren.
When to Suspect NPH
If you or someone you know over 60 has:
- Shuffling, slow, wide-based walking
- Memory lapses that don’t fit typical Alzheimer’s patterns
- Loss of bladder control without other causes
-then ask for a neurology referral. Push for an MRI and a CSF tap test. Don’t accept “it’s just aging.” NPH is rare, but it’s treatable. And the window to fix it? It’s narrow. Studies show if you wait more than 12 months after symptoms start, the chance of full recovery drops by 30%.
One man in Perth, 74, walked into his GP’s office in 2023 saying, “I can’t get out of my chair anymore.” He’d been told he had dementia. After a CSF tap test, he improved instantly. He had a shunt. Three months later, he was gardening again. He didn’t get better because he got older. He got better because someone finally looked.
Is normal pressure hydrocephalus the same as Alzheimer’s?
No. Alzheimer’s mainly affects memory and language, with gait problems appearing only in late stages. NPH starts with walking problems, followed by thinking changes. MRI scans show different brain patterns. And unlike Alzheimer’s, NPH can be reversed with surgery.
Can NPH be cured with medication?
No. There are no drugs that remove excess cerebrospinal fluid or reverse brain compression in NPH. Surgery with a shunt is the only proven treatment. Medications for dementia, like cholinesterase inhibitors, don’t help NPH symptoms.
How do I know if I’m a candidate for a shunt?
You need to meet three criteria: 1) Symptoms of gait, cognition, or bladder issues lasting more than 3 months; 2) MRI showing enlarged ventricles with no other cause; 3) Improvement after a CSF tap test or external drainage. If you don’t improve during the test, you’re unlikely to benefit from a shunt.
What are the risks of shunt surgery?
The most common risks are infection (8.5%), shunt malfunction (15% within 2 years), and bleeding around the brain (5.7%). Overdrainage can cause headaches. Most complications can be fixed with adjustments or revisions. The risk of not treating NPH-losing independence-is often higher.
How long does it take to recover after shunt surgery?
Most people go home in 2-3 days. Walking improves within days to weeks. Full recovery takes 6-12 weeks. Cognitive changes may take longer to improve-sometimes up to 6 months. Physical therapy helps speed up progress. Regular follow-ups with a neurosurgeon are essential.
Can NPH come back after surgery?
The condition doesn’t “come back,” but the shunt can fail. Shunts last an average of 6.3 years before needing repair or replacement. About 32% of patients need at least one revision. Long-term symptom improvement is seen in 68% of patients after 20 years, according to Swedish registry data.
Is NPH covered by Medicare?
Yes. Medicare covers shunt surgery and diagnostic tests like MRI and CSF tap tests if they meet clinical guidelines. However, prior authorization is often required, and some insurers deny coverage for lumbar drainage. Patients should work with their neurologist to document symptoms and test results to support approval.
rajaneesh s rajan
January 29, 2026 AT 06:26Keith Oliver
January 30, 2026 AT 00:46Insurance denies it 37% of the time. That’s not a glitch. That’s systemic neglect.
Kacey Yates
January 31, 2026 AT 23:17Doug Gray
February 2, 2026 AT 00:45And the shunt? A technological prosthetic for the neglected cerebral aqueduct. We are literally plumbing the mind.
DHARMAN CHELLANI
February 2, 2026 AT 05:22Pawan Kumar
February 3, 2026 AT 20:22kabir das
February 4, 2026 AT 21:59ryan Sifontes
February 6, 2026 AT 03:07paul walker
February 7, 2026 AT 08:17Alex Flores Gomez
February 8, 2026 AT 10:38Laura Arnal
February 8, 2026 AT 16:15Frank Declemij
February 9, 2026 AT 15:27