Kyphoplasty vs Vertebroplasty: Which Vertebral Fracture Treatment is Right for You?
 Apr, 13 2026
Apr, 13 2026
Imagine waking up with a pain in your back so intense that you can't even sit up in bed. For many people, especially those dealing with osteoporosis, a vertebral compression fracture isn't just a medical diagnosis-it's a sudden loss of independence. When bracing and painkillers aren't enough, the conversation usually turns to two minimally invasive procedures: Kyphoplasty and vertebroplasty. While they sound similar and both use medical-grade cement to stabilize the spine, the way they handle your vertebrae is quite different. The goal for both is simple: stop the bone from collapsing further and get you back on your feet without a massive open surgery.
The Basics of Vertebral Augmentation
At their core, both of these procedures belong to a category called vertebral augmentation. They are designed to treat fractures caused by Osteoporosis, trauma, or cancer that has spread to the bone. Instead of a large incision and a long hospital stay, these are "percutaneous" procedures, meaning the surgeon uses a needle or a small tube (trocar) to reach the bone through the skin.
The "secret sauce" for both is Polymethylmethacrylate (PMMA), a fast-hardening bone cement. This cement acts like a structural cast inside the bone. Once it's injected, it hardens in about 10 to 20 minutes, providing immediate stability to the fractured vertebra. For most patients, the relief is almost instant; many see their pain scores drop from a severe 8 out of 10 to a manageable 1.5 within the first 24 hours.
Vertebroplasty: The Direct Approach
Think of Vertebroplasty as the straightforward version of the process. Developed back in 1984 in France, this method is purely about stabilization. The surgeon uses a real-time X-ray (fluoroscopy) to guide a needle directly into the collapsed part of the vertebra. Then, they inject the PMMA cement under relatively high pressure-usually between 150 and 200 psi.
Because the cement is pushed directly into the porous, cancellous bone, it locks into place quickly. The whole process usually takes between 30 and 60 minutes. While it's incredibly effective at stopping pain, it doesn't do much to fix the "shape" of the bone. If your vertebra has collapsed and left you leaning forward, vertebroplasty will stop the pain and the collapse, but it won't push the bone back up to its original height.
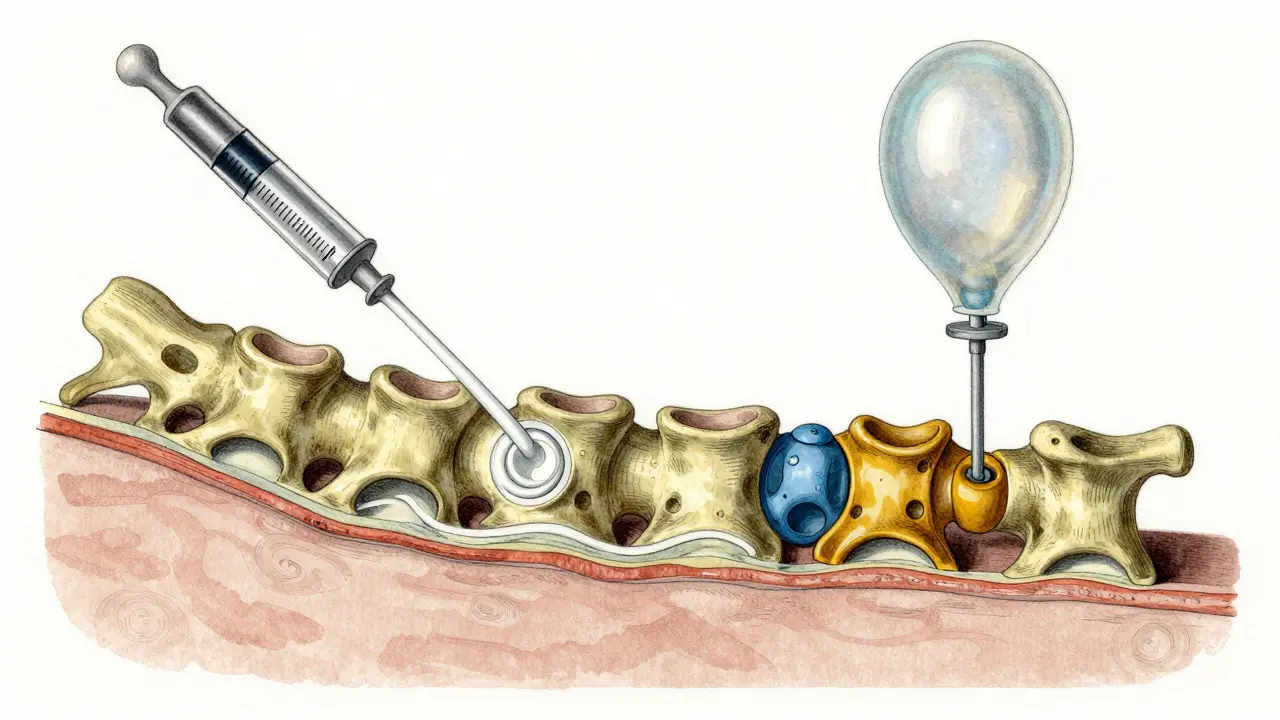
Kyphoplasty: The Balloon Technique
If vertebroplasty is a direct injection, Kyphoplasty is more like a controlled renovation. It adds a critical step: the balloon. Before any cement is added, the surgeon inserts a small orthopedic balloon (roughly 8-15mm) into the fractured space.
This balloon is inflated with saline to about 200-300 psi. This does two things: it creates a cavity (usually 2-4cc in volume) and, more importantly, it can actually lift the collapsed bone back up. Biomechanical data shows that kyphoplasty can restore about 40% to 60% of the lost vertebral height. Once the height is restored, the balloon is deflated and the cement is poured into the newly created cavity.
This "controlled cavity" is a big deal for safety. Because the balloon creates a space for the cement to go, there's less pressure pushing the cement outward. This reduces the risk of cement leaking into surrounding areas-a complication known as extravasation-by about 40% compared to the direct injection method.
| Feature | Vertebroplasty | Kyphoplasty |
|---|---|---|
| Primary Goal | Pain relief & stability | Pain relief, stability & height restoration |
| Method | Direct cement injection | Balloon inflation followed by cement |
| Height Restoration | Minimal | Significant (40-60% average) |
| Cement Leakage Risk | Higher (27-68%) | Lower (9-33%) |
| Average Cost | Lower (~$2,950 Medicare rate) | Higher (~$3,850 Medicare rate) |
Which One Should You Choose?
The choice usually comes down to the specific nature of your fracture and your goals for recovery. If you have a stable fracture that is causing intense pain but hasn't changed the shape of your spine much, vertebroplasty is often the most cost-effective and efficient path. It's a "value" play-similar pain relief for a lower price tag.
However, if you have significant height loss (over 30%) or a noticeable "hunch" (kyphotic deformity), kyphoplasty is the clear winner. It's the only one of the two that can actively fight the deformity. While some studies, like the one by Baroud et al., suggest that these height gains can diminish over time as the spine undergoes thousands of loading cycles, the initial correction can be vital for long-term mobility and breathing capacity.
From a safety perspective, kyphoplasty is generally viewed as safer for patients with very poor bone quality because the balloon prevents the cement from simply "shooting" through the bone into the bloodstream or spinal canal. While serious complications like pulmonary embolisms are rare for both (around 0.6% to 1.1%), the lower leakage rate of kyphoplasty provides an extra layer of security.
What to Expect During and After the Procedure
Regardless of which path you take, the experience is remarkably similar. You'll be positioned face-down (prone) and will likely receive local anesthesia with IV sedation. You aren't usually spending the night in a hospital; the vast majority of patients go home the same day.
The recovery is surprisingly fast. About 92% of patients return to their normal daily activities within 72 hours. One of the most impactful outcomes is the reduction in medication; roughly 75% of patients are able to stop taking opioids within a week of the procedure because the mechanical source of the pain has been fixed.
There are a few pitfalls to watch for. About 5-10% of patients may experience a new fracture in the vertebrae directly above or below the one that was treated. This happens because the treated vertebra becomes very rigid (thanks to the cement), which puts more stress on the softer, untreated bones neighboring it. To minimize this, it's crucial to continue treating the underlying osteoporosis with medication and physical therapy.
The Path Forward: New Tech and Trends
The field isn't standing still. We're seeing a move toward Calcium Phosphate Cements. Unlike PMMA, which is essentially a hard plastic, calcium phosphate better mimics real bone. This reduces the risk of thermal damage to the surrounding tissue and may allow the body to integrate the material better.
There's also a growing push for "early intervention." The Vertos II trial indicated that treating a fracture within the first two weeks can actually reduce 12-month mortality by 28%. This is a huge shift; in the past, doctors often waited weeks for conservative treatment to fail. Now, the evidence suggests that acting fast can save lives by preventing the "downward spiral" of immobility that often follows a spinal fracture in the elderly.
Does the cement last forever?
Yes, the PMMA cement used in these procedures is permanent and does not dissolve over time. It provides a lifelong structural support for the fractured vertebra, though it's important to note that this can make the treated bone stiffer than its neighbors, potentially increasing the risk of future fractures in adjacent vertebrae.
Will I need to stay in the hospital overnight?
In most cases, no. Both kyphoplasty and vertebroplasty are typically outpatient procedures. After a few hours of monitoring to ensure the anesthesia has worn off and there are no immediate complications, most patients are discharged the same day.
Is there a risk of the cement leaking?
There is a risk, but it's generally low. Cement leakage is more common in vertebroplasty (27-68%) than in kyphoplasty (9-33%). However, the vast majority of these leaks are "asymptomatic," meaning they don't cause any new symptoms. Only about 0.6% to 1.1% of patients experience clinically significant complications from leakage.
Can these procedures cure osteoporosis?
No. These procedures treat the result of osteoporosis (the fracture), not the disease itself. You will still need to work with your doctor on a systemic treatment plan-such as bisphosphonates or other bone-building medications-to strengthen your other vertebrae and prevent new fractures.
How soon can I walk again?
Most patients are encouraged to begin light walking almost immediately. While you'll have some weight-bearing restrictions for the first 24 hours, the majority of people return to their normal daily activities within 72 hours of the procedure.
Next Steps and Troubleshooting
If you suspect you have a vertebral fracture, the first step is an MRI. This is the only way to confirm that a fracture is "acute" (meaning it has active inflammation or bone marrow edema). These procedures are not meant for old, chronic fractures that have already healed into a collapsed shape.
For those who have already tried a back brace for 4 to 6 weeks without relief, it's time to ask your specialist about "augmentation." If you're worried about the cost, check if your insurance or Medicare covers the procedure; approval rates are typically over 95% when a history of failed conservative management is documented.
If you experience new, sharp pain in a different part of your back after a successful procedure, don't panic, but do get it checked. As mentioned, "adjacent level fractures" are a known risk, and catching them early allows for the same quick-fix treatment to be applied to the new site.